
Aug 27, 2021
By Stephanie Schorow for the Global Mass Vaccination Site Collaborative
Benjamin D. Trump, PhD, a research social scientist for the U.S. Army Corps of Engineers, began his presentation to the Global Vaccination Site Collaborative on his efforts to document inequities in COVID vaccination as he would a military briefing “with the bottom line up front.”
There is, he first acknowledged, “no such thing as perfect data collection with COVID.” Too much of the reporting remains incomplete.” Yet utilizing census data, the initial supply chain for vaccines, and other information, Trump was able to create a portrait of where the United States stands in terms of working toward achieving herd immunity.
Since March 2020, at the behest of FEMA, Trump and Dr. Igor Linkov, a senior scientific technical manager with the U.S. Army Engineer Research and Development Center, have worked to create a methodology to assess and compare vaccine equity within and across regions. President Biden has asserted that equal opportunity in vaccine access is critical to COVID-19 recovery. Public health officials need ways to benchmark and prioritize information to promote equitable access.
Trump and team focused on three questions: Does vaccine inequity exist, where does it exist, and why does it persist? The answer to the first question was clearly “Yes,” and data could pinpoint inequity county by county. As for the “why,” Trump discussed the issue of “vaccine hesitancy as a proxy for lack of access because the data for the latter is not great.”
Hesitancy has been decreasing in response to the Delta variant, but hesitancy remains high in the subgroup of individuals who have only received the first shot of the two-shot vaccines, Trump said. This group is small but poses worries for achieving herd immunity. There are “an awful lot” of reasons for hesitancy, he noted, but chief among them is the fear of side effects. Others adopt a “wait and see” attitude about the vaccine’s safety over time, a concern that may not be mitigated by the FDA’s recent approval of the Pfizer vaccine. Others simply mistrust the government.
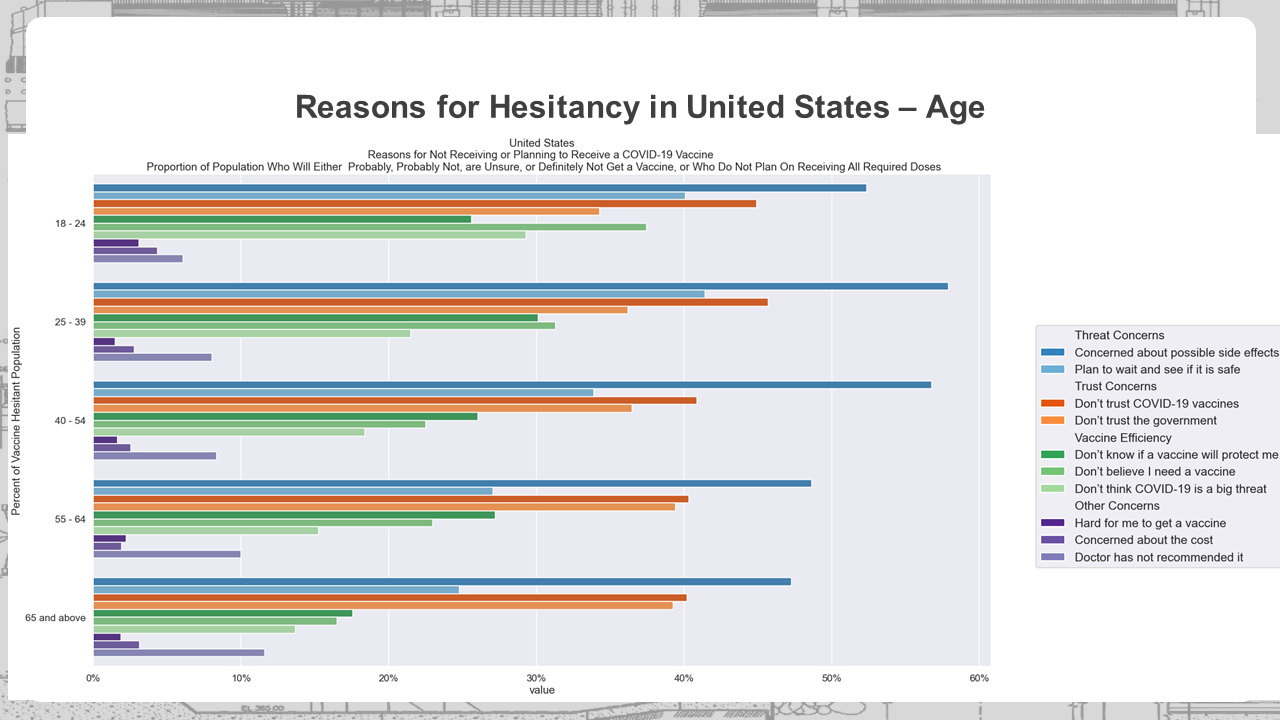
As Julie Rosenberg, MPH, Assistant Director of Project Management, Better Evidence at Ariadne Labs, noted in the Zoom chat, Washington State data from unvaccinated groups indicated that FDA approval won’t change their intentions as they have overall lost trust in the FDA based on its speed and handling of the vaccines. Another collaborative member in the chat noted that religious conviction may have an effect as “some religious/spiritual individuals have not yet received an individual instruction from God to get vaccinated.”
There also is confusion over the difference between infection and hospitalization rates and thus over the vaccine’s efficacy. “A good amount of folks are saying, ‘Maybe I don’t need the vaccine,’ ” Trump said. Many conflate the concept that “boosters will help efficacy” with “vaccines don’t work at all.”
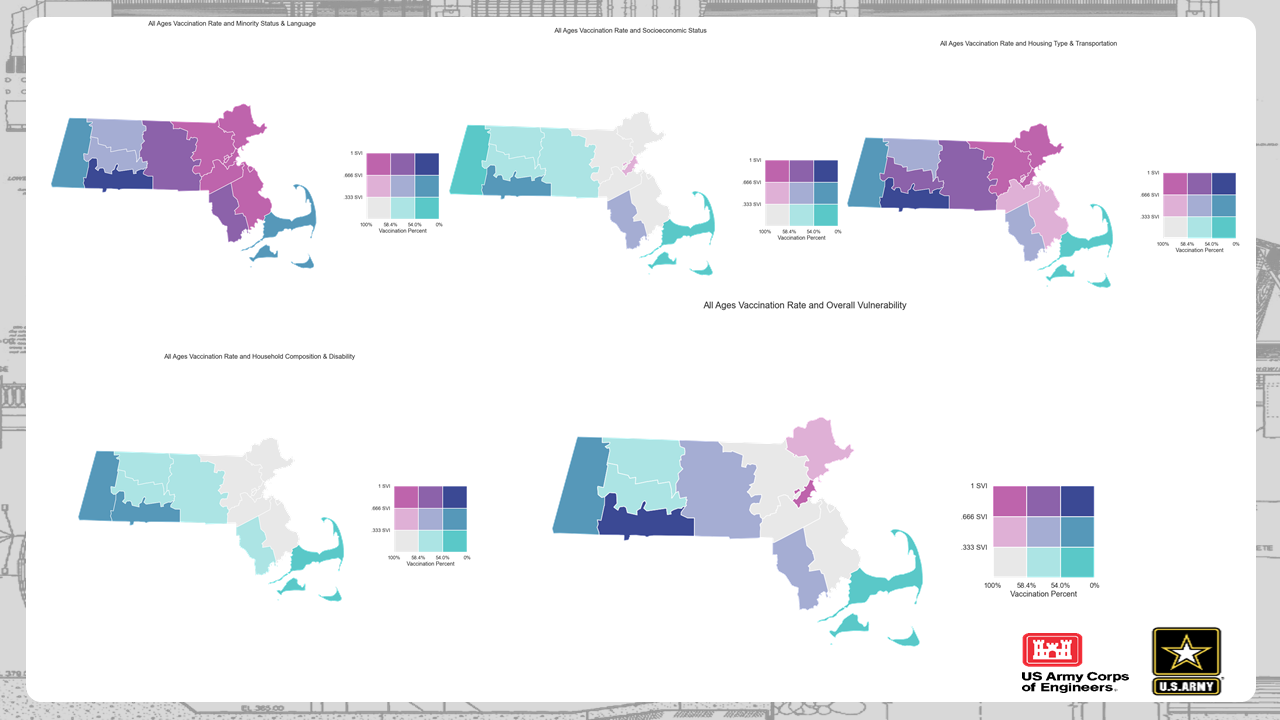
People with higher incomes tend to be more vaccinated; vaccination rates decline with income as low-income, single-parent households, and young individuals without insurance worry about losing pay because they would have to miss work to get vaccinated. Using the CDC’s Social Vulnerability Index, Trump’s team found areas of vaccine inequity in places with issues with housing and transportation, thus pinpointing opportunities for closing gaps.
Eric Goralnick, MD, MS, Associate Faculty, Ariadne Labs and Principal Investigator of the Global Vaccination Site Collaborative, praised Trump’s meticulous presentation and commented that the information was like “snapshots in time.” He asked Trump if he had thought about mapping out the impact after policy changes. “We have definitely thought about it,” Trump said, indicating it is a question his team would be interested to explore. Becky Fox, MSN, RN-BC, of Atrium Health also wondered about the community-wide effect of local school mask policies. Trump said this might also be tracked.
While numbers don’t tell the whole story of COVID-19, this data could be used to develop effective strategies to promote further uptake of the COVID-19 vaccines.
Key Takeaways
- Vaccine hesitancy has many roots but the dominant one is fear of side effects.
- Those who adopt a “wait and see” attitude will be much harder to convince than those concerned about side effects.
- The Delta variation is having an effect on decreasing hesitancy.
- More education is needed about infection rates versus hospitalization rates to show that the vaccines are, indeed, having an effect on saving lives.
- A high Social Vulnerability Index seems correlated with a lower vaccination rate, which may help to devise more effective interventions.
The Global Mass Vaccination Site Collaborative was launched as a way for stakeholders directing vaccination campaigns around the world to come together and learn from each other’s efforts. This blog series was created to record and share the learning and insights gained from this collaboration. Read blogs from our previous meetings here.