
Overview
Ariadne Labs, a joint center for health systems innovation at Brigham and Women’s Hospital and the Harvard T.H. Chan School of Public Health, seeks partnerships with states, or individual rural hospitals, to provide an opportunity for their rural hospitals to participate in a Rural Home Hospital (RHH) Accelerator project. The Accelerator will provide expertise in designing and launching home hospital programs via a network of hospitals that collectively learn, create, and implement together as a community. States (with rural hospital(s)) or individual hospitals that want to participate will submit applications showcasing interest, readiness, and financial buy-in. States and hospitals should reach out to partner on applications for Rural Health Transformation funds from their state.
Accelerator Timeline
| Schedule | |
| Scrum Accelerator | Months 1-9 |
| Home Hospital Program Launch | Month 10 |
| Evaluation | Months 10-18 |
Ariadne Labs will set the dates of accelerator cycles with interested rural hospitals and states to meet their readiness and needs.
Eligibility and Costs
Eligibility:
- Any state with a general hospital located in a rural location
- A general hospital located in a rural location
Approximate Cost:
Proposals for Rural Health Transformation funds would request approximately $1,500,000 per hospital participating in the accelerator. $1,000,000 provided to the hospital directly and $500,000 to Ariadne Labs.
Background
Access to high quality, high value acute care services in rural communities is a growing national problem. About 1 in 5 Americans live in rural areas, totaling nearly 60 million people. An acute illness that traditionally requires hospitalization represents a common critical moment in nearly every person’s life. While some face intense travel burdens to obtain acute care, others simply go without. America’s rural hospitals are struggling to remain open or are closing; the cost to support traditional rural hospital infrastructure is unsustainable. Between 2011 and 2017, the average daily census for rural hospitals declined by 13%. Balancing the high cost of hospital infrastructure with the low volume of acutely ill patients is difficult from a fiscal and readiness perspective. Approximately 41% of rural hospitals operate at a negative margin. As a result, the rate of rural hospital closures is increasing, with over 150 rural hospitals closing between 2005 and 2024. Quality and safety of acute care in rural settings are often poor: Even when a rural community has a hospital, that hospital, in the aggregate, performs poorly compared to its urban counterpart, resulting in increased morbidity and mortality. Poor quality care results in high rural hospital bypass rates to larger urban facilities. Hospital bypass rates average from 25% to 70%.
Roles & Responsibilities
Ariadne Labs: will provide continuous RHH clinical, operational, and research expertise to support each hospital to design, launch, and manage the project at each site, as detailed above. This support will include access to home hospital knowledge products, a network of home hospital experts to connect with for support throughout the development and launch of the rural home hospital, technical expertise, and agile training and coaching. Ariadne Labs will also evaluate the impact of the Rural Home Hospital program, providing impact metrics data as required by RHT.
State Office: will provide the financial support with Rural Health Transformation funds, $1,500,000 per hospital required – $1,000,000 directly to each hospital to catalyze the development, launch, and early implementation. They will also provide the funding to Ariadne Labs to run the Accelerator and support their hospital(s) in launching home hospital programs – $500,000 per hospital.
Rural Hospital Sites: will provide the time and expertise of staff to engage with the Ariadne Labs team to tailor, launch, manage, and review the Rural Home Hospital program. Sites will collaborate closely with Ariadne Labs who will lead Scrum Sprints that will produce site assessments, protocol development, and technology procurements plans. Sites will execute procurement plans and provide staff to participate in the Accelerator and staff their rural home hospital program.
Rural Home Hospital Accelerator Model
The primary outcome of the Accelerator will be home hospital program launch.
The Ariadne team will provide expertise in designing and managing home hospital programs via a network of hospitals that collectively learn, create, and implement together as a community. As we have done in the past, rural hospital sites will be selected through a competitive process that will assess their readiness for RHH deployment, leadership buy-in, and contextual factors that will contribute to effective collaboration with Ariadne Labs and a high likelihood of home hospital launch.
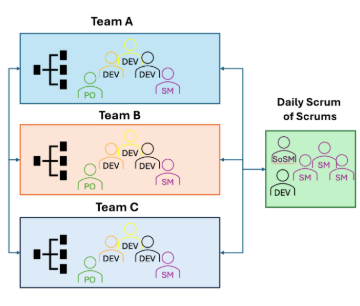
The accelerator will use the Scrum framework (Figure 1) for agile product development – and with participation from a number of hospitals will leverage the Scrum at Scale model (Figure 2) to allow for parallel sprints – or products to be worked on simultaneously. This model will allow for mixed teams from different hospitals working toward the same goal with oversight and support to alleviate impediments from an Ariadne Labs based scrum master and scrum of scrum master. In addition to the role of scrum master, Ariadne Labs would provide product owners for these teams to provide guidance and leadership to better understand the product’s end goal.
The accelerator will be based on the Rural Home Hospital Implementation Roadmap. It will be refined with input from participating accelerator hospitals after the selection process and before launch of the accelerator.
By the end of the Accelerator, participating accelerator hospitals will launch home hospital programs at their individual hospitals. Once programs have been launched, participating hospitals will complete surveys and interviews at implementation and 3- and 6-months post implementation to inform about the success of the programs. We will measure patient volume, escalation rate, and mortality, among other metrics.
To complete the project, Ariadne Labs will analyze the data and stories on the experience and impact of the RHH accelerator. We will work to disseminate information through media outlets, relevant healthcare associations, and peer-reviewed journal. We anticipate this Accelerator will spawn a transformation in how acute care is delivered in rural areas, clarifying a path for more rural hospitals to move to the RHH model. Of note, sites must be open to patient-level data sharing agreements.
Figure 1. Scrum Framework
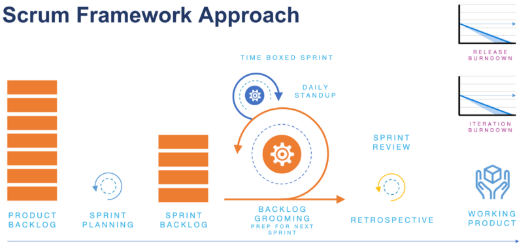
Figure 2. Scrum at Scale Model Example
Learn More
Watch our informational webinar to learn more about Ariadne Labs’ expertise and the Rural Home Hospital Accelerator
Ariadne’s Expertise
Our team has worked for years to bring acute care home through the “home hospital” model. Despite the success of home hospital programs, few operate in rural areas, where an opportunity exists for outsized impact. In recognition of the geographic disparities in access and quality of care, and financial distress of rural hospitals across the US, Ariadne Labs launched the Rural Home Hospital (RHH) project in November 2018 to adapt urban home hospital principles and implement innovative technologies, top-of-license personnel, and novel workflows to deliver high-value acute rural care. Through a feasibility pilot and then a multisite randomized control trial the team implemented these technologies and protocols. In the randomized controlled trial, the team found lower costs for patients who start care at home quickly, similar safety and quality outcomes, with significantly higher patient and caregiver satisfaction.
Hospital-Level Care at Home for Adults Living in Rural Settings: A Randomized Clinical Trial | JAMA Network Open
Home Hospital Care Demonstrates Success in Rural Communities
Outcomes from an Early Adopters Home Hospital Accelerator for Acute Care at Home | JGIM
Frequently Asked Questions
What is the Rural Home Hospital Accelerator?
The Rural Home Hospital Accelerator is a fused network of rural hospitals learning together to build and implement a home hospital program for acute care at home. The program will provide expertise in designing and managing home hospital programs via a network of hospitals who collectively learn, create, and implement together as a community. Products and implementation plans will be developed over 20 two-week sprints using an adapted Scrum framework for agile product development.
What does the time commitment look like?
Throughout the accelerator representative(s) from the hospital will need to join every two-week sprint. During a sprint, a daily 15-minute meeting will be required, in addition to working in small groups throughout the two weeks. We estimate about three to four hours of work each week. As the accelerator builds towards launch of the home hospital program, we anticipate that broader and more time intensive participation will be needed. Once the home hospital program launches the time commitment to the accelerator program reduces to survey and interview completion and data sharing on a quarterly basis to support measuring success.
Who will need to be involved in each sprint? Will team members involved in each sprint need to be topic focused?
It would be great if your hospital/health system could commit one to two individuals who will join every/most sprints your organization participates in, with the addition of one to two team members who will join sprints based on their area of expertise. For example, if a sprint has a pharmaceutical focus, including someone from your organization’s pharmacy team in the sprint would enrich the experience and the development of the knowledge product.
What are some examples of scrum topics that will be covered during the accelerator?
Some topics that may be included: Numbers and Pre-Implementation Plan, Personnel, Protocols, Workflows, Supplies, Transportation, Compliance, Measures, Payors, Communication, Training, Simulations, Launch
What is the cost to participate in the accelerator?
There needs to be a commitment of funds of $1,500,000 for each participating hospital, funds from the Rural Health Transformation Program are a useful resource. Participating hospitals should directly receive $1,000,000 to compensate for staff time needed to participate in the accelerator to develop and launch home hospital and then $500,000 to Ariadne Labs to run the accelerator.
How long does the accelerator last?
Hospitals are required to be engaged for 18-months; the first 9 months will be participating in the sprints, building towards implementing their own home hospital program. Following implementation, hospitals will continue to be engaged with coaching, completing surveys, sharing data, and contributing to measuring the success of the accelerator and their home hospital program.
Have additional questions? Please reach out to Annie Rushman (arushman@bwh.harvard.edu).