We found 256 results for your search.
The Delivery Decisions Initiative publish results in the Journal of Nursing Management where they sought to measure the association between job satisfaction and perceived quality of care among nurses on labor and delivery (LD) units.
Our Eldercare Team’s published results in JAMDA from their 6-month pilot in 2 rural nursing homes to assess feasibility, acceptability, and utility of the Wellbeing Toolkit.
The BetterBirth Team and their partners at KEMRI Wellcome Trust and the University of Oxford published the results from their mixed methods study at three county referral hospitals in Kenya to explore the impact of birth complications on mothers’ and families’ postpartum experiences and wellbeing.

A randomized controlled trial, published in JAMA Network Open and led by Ariadne Labs, showed that Rural Home Hospital programs can deliver acute care at an equal or lower cost compared to brick-and-mortar hospitals, while providing a better patient experience.
TeamBirth publishes findings from our partnership with the state of Oklahoma that shows that patients who experienced a TeamBirth huddle during labor was associated with increased patient trust and autonomy scores.
The International Consortium of Newborn Sequencing (ICoNS) published their findings and tool in Genetics in Medicine. They identified key factors influencing gene inclusion in newborn genomic screening programs and the team developed a machine learning model incorporating 13 predictors, achieving high accuracy in predicting gene selection across programs.
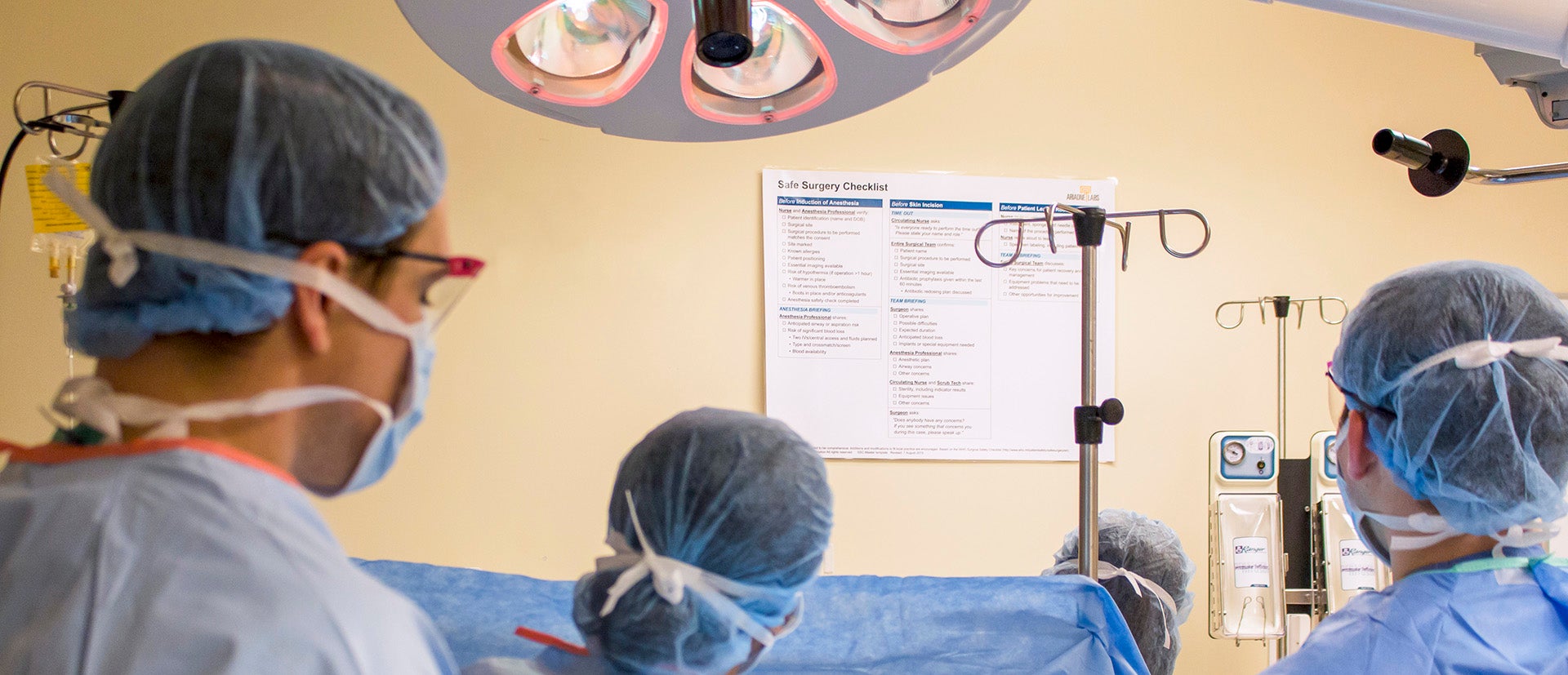
The Safe Surgery/Safe Systems team publish their conceptual framework for team-based morbidity and mortality conferences in The Joint Commission Journal on Quality and Patient Safety.
Published results from the Spark Grant program’s Cultural Brokering project explores the role that cultural brokers fulfill during pregnancy care for patients with limited English proficiency and the need to recognize, value, and integrate cultural brokering into pregnancy care.

National Academies release new report, co-chaired by Dr. Asaf Bitton, making specific recommendations for CMS, to address the systemic flaws currently affecting primary care professionals and limiting the potential of high-quality primary care services for all.
The Spark Grant-funded Stroke Checklist team published their results on a 2-year quality improvement project co-designed and tested a checklist for quicker evaluation of suspected stroke cases in two emergency departments.
